Sachchidanand Pathak*, Gaurav Gupta, Ritu M Gilhotra
Gyan Vihar School of Pharmacy, SGVU Jaipur, INDIA
INTRODUCTION
Benzodiazepines (BZDs) are one of a kind and are the most broadly depicted drug on the planet. BZDs are utilized for a few pointers, to compute nervousness, a sleeping disorder, muscle unwinding, help from pressure brought about by focal sensory system pathology, and epilepsy. BZDs are additionally utilized intraoperatively in light of their amnesic and anxiolytic properties. In spite of the fact that, these properties have undesirable reactions in practically completely broadened times of treatment.
Unhindered unfriendly impacts of BZD brought about by furnished specialists to make nervousness and consideration the symptoms when choosing this class of agents. Resistance, reliance, age-related physical changes, and medication collaborations are largely factors to consider[1,2].
Benzodiazepine Pharmacology
General/Pharmacodynamics
BZDs go about as fine allosteric modules in the gamma-aminobutyric corrosive (GABA)- receptor. The GABA-A receptor is an igand-gated chloride-determination particle channel.
GABA is the most widely recognized synapse in the focal sensory system, which is found with high fixations in the cortex and the limbic framework. GABA is inhibitory and hence lessens the volatility of neurons. GABA creates a cooling impact on the cerebrum. GABA receptors are known as A, B, and C. This article centers explicitly around the GABA-A receptor, where BZDs communicate.
The GABA-A receptor complex is made out of 5 glycoprotein subunits, each with numerous isoforms (Figure 1). GABA-A receptors contain 2 ′ subunit, 2 β, and 1 γ subunit. Every receptor complex contains 2 GABA-restricting destinations however just 1 BZD site. The benzodiazepine restricting site is situated in a particular pocket in the mating (surface intersection) of α and un subunits. Inside the α subunit of isoforms 1, 2, 3, and 5 stay a histidine buildup (H101, H101, H126, and H105, individually) with a high liking for BZDs. Isoforms 4 and 6 of the sub subunit contain arginine deposits and have no relationship of BZDs. BZDs tie to the pocket made by α and γ and initiate secretory changes in the GABA-A receptor, permitting GABA official. BZDs that quandary to the pocket are made by α and γ and incite discharged changes in the GABA-A receptor. This transformation, instigates an emitted change in the chloride channel of the GABA-A receptor by hyperpolarizing the cell and afterward ascertains the GABA’s inhibitory impact all through the central nervous system [3,4].
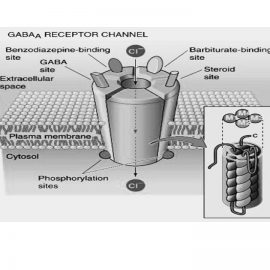
Fig: 1- GABAReceptor
The BZD receptor is separated into a few sorts, in view of the isoforms of the α subunit and the clinical impacts related with each kind. The BZ1 receptor contains the α1 isoform. The BZ1 receptor is profoundly packed in the cortex, thalamus, and cerebellum, answerable for the impacts of narcotic BZDs and anterograde amnesia and other anticonvulsive impacts of diazepam. 60% of GABA-A receptors contain the α1 subunit. Along these lines, amnesia is a typical outcome of BZD use in light of the fact that the vast majority of the GABA-A receptors contain the BZ1 receptor answerable for amnesia. A central point in foreseeing the danger of amnesia is lipid dissolvability; the more lipid solvency, the more the danger of amnesia. BZDs with higher lipid dissolvability have higher incorporation rates and quicker beginning of clinical results than BZDs with lower lipid solubility.
BZ2 receptors contain the α2 isoform4 and anxiolytic linker and, to an enormous degree, the myorelaxant impacts of BZDs.6 BZ2 receptors are basically gathered in zones, for example, the limbic framework, engine neurons, and dorsal spinal string. . The tension impacts of BZDs are accepted to be interceded by the BZ2 receptors found in the limbic framework, and the properties of myorelaxant are partitioned into receptors containing α2 in the spinal line and engine neurons. Not all BZDs share a similar kind of BZ receptor or are similarly touchy to a particular receptor. These varieties in the α subunit isoforms, the kind of BZ receptor enrollment, and our area inside the sensory system represent various impacts of the different BZDs [4].
Benzodiazepine Pharmacokinetics
The pharmacokinetic properties of a medication decide the beginning of activity and the length of its impact. Specifically, pharmacokinetics portrays the assimilation, appropriation, digestion, and discharge of a medication. Pharmacodynamics portrays the reaction of receptors to a medication and the instrument by which these impacts happen. Various people respond contrastingly to a similar medication, and regularly these various reactions reflect pharmacokinetics and/or pharmacodynamics in various patients.
Pharmacokinetics (deciding the beginning of activity and length of medication impacts) is affected by the course of organization, retention, and conveyance volume. BZDs can be directed by means of intramuscular, intravenous, oral, sublingual, intranasal, or rectal gel structures. Attributes of the medication – including lipid dissolvability, authoritative to plasma proteins, and atomic size – influence the measure of conveyance. Pharmacodynamics and pharmacologic medication impacts are portrayed as far as portion reaction bends that mirror the relationship among portion and the subsequent pharmacologic impact. Portion reaction bends anticipate the impact of the medication on the patient when the portion is expanded.
Previous influences the half-life at end of ailment procedures and age-related changes, particularly significant while controlling BZDs. The disposal half-life is the time required to decrease the plasma centralization of a medication to half during the end stage. Since end is straightforwardly corresponding to the measure of half-life dispersion and its freedom is conversely relative to kidney and liver infection, end influences half-life. The disposal half-life doesn’t mirror an opportunity to recuperate from the impacts of the medication. The end half-life is a gauge of the time required to lessen the medication focus in plasma. After around 5 disposal half-lives, around one medication is wiped out from the body. Accordingly, there is a chance of medication amassing if there is a short stretch from this period[4-6].
From a pharmacological perspective, BZD is commonly all around consumed by the gastrointestinal tract after oral organization. After intravenous organization, BZDs rapidly convey to the mind and focal sensory system. BZD movement is abrogated by redistribution like lipid-solvent barbiturates. After intramuscular infusion, retention of diazepam or chlordiazepoxide is moderate and dubious, while ingestion of intramuscular organization of lorazepam or midazolam seems, by all accounts, to be quick and complete. Lorzepam is all around ingested after subal organization, arriving at top levels in an hour.
BZDs and their metabolites are profoundly protein-bound. They are generally circulated in the body and ideally gather in lipid-rich areas, for example, the focal sensory system and fat tissue. As noted before, progressively lipophilic operators for the most part have the most elevated pace of ingestion and the quickest beginning of clinical impacts. Most BZDs are oxidatively used by cytochrome P450 chemicals, which are conjugated to glucuronide, and are as a rule discharged in pee.
Some BZDs make extra move through the creation of dynamic metabolites, a significant thought while deciding these specialists. Midazolam, one of the short-acting BZDs, delivers no dynamic metabolites. Be that as it may, diazepam, a long-acting BZD, produces dynamic metabolites oxazepam, desmethyl diazepam, and temazepam; These metabolites further increment the length of medication activity and ought to be a genuine thought in some patient gatherings, particularly the older and individuals with broad liver illness[7,8].
Benzodiazepines in clinical practice
Short-acting BZDs have a normal end of 1–12 hours, middle of the road acting BZDs have a normal end half-existence of 12–40 hours, and long-acting BZDs have a normal disposal half-existence of 40–250. Hours occur. As referenced before, 5 half-lives are typically required to clear off an operator’s body, A medication shaft contains the quantity of hours in the body.
Another approach to characterize BZDs is relative force. The first BZDs were low to medium force. These incorporate the long-acting chlordiazepoxide, the first BZ to be found, just as oxazepam and temazepam. As a result of their adequacy and low poisonousness, they have become first-line specialists for conditions, for example, a sleeping disorder and uneasiness. In this manner, high-potential BZDs (alprazolam, lorazepam, and clonazepam) were found. These new medications offer new signs for use: as a treatment for alarm issue, particular serotonin reuptake inhibitors for the treatment of over the top impulsive issue, and as an aide to antipsychotics for the treatment of serious lunacy or uneasiness. Structure. New high-effectiveness BZDs have indicated the fast beginning of activity, alongside restorative impacts, which have become the favored BZDs for most applications. In any case, the danger of undesirable impacts increments with expanded effectiveness. Thusly, when recommending drugs in this BZD gathering, clinicians ought to consider various attributes, for example, ingestion, dispersion, end half-life, and lipid solvency[9,10].
Alprazolam
Alprazolam is a little acting high-effectiveness BZD that has an end half-existence of 6–27 hours. Alprazolam was first read for use in alarm issue and end up being all around endured and compelling. Alprazolam is generally endorsed for fears and tension. The suggested portion for uneasiness begins with 0.25–0.5 mg tablets, given orally 3 times each day. The every day suggested portion of alprazolam for apoptosis ought not surpass 4 mg. For apprehensive scatters, a most extreme portion of 6-10 mg/d is suggested in a solitary pill structure and course of organization. A typical issue with alprazolam is the beginning of a rebound of uneasiness, which suddenly stops because of the short end half-existence of the drug.
Diazepam
Diazepam is a protracted-acting, medium-energy BZD used as an anticonvulsant and for angiolytic, anesover the countertic, and myorexation. Diazepam, over-the-counter maximum common BGDs used for anxiety, is to be had in intramuscular, intravenous, oral, and anal gel paperwork. Diazepam interacts with similar affinity in any respect BZD-sensitive receptors of over-the-counter significant apprehensive device. Inside over the counter limbic device of diazepam, angiolytic outcomes appear in small quantities due to interactions with α2-containing receptors. At better doses, diazepam may additionally provide myorexation similar lyover the counter to angiolytics; The spinal wire impact is mediated over-the-counterr over-the-counter α2-containing receptors over-the-counter over the counter spinal twine and motor neurons, and over-the-counter interactions with αthree-containing receptors. In truth, at higher doses, morphine and anisotropic amnesia are also detected, but those results are α1-mediated. Diazepam is particular over the counter experience that its metabolism inside ove the counter liver produces active metabolites consisting of oxazepam, temazepam and desmethyl diazepam, every of which regulates its pastime. those metabolites and over-the-counterir actions purpose lengthy-time period elimination of diazepam, which increases to about 1 hour each yr older than 40 years (eg, elimination 1/2-life of diazepam at age seventy five is ready seventy five hours). over-the-counterrefore, whilst prescribing this drug, physicians ought to consider over-the-counter facet results related to lively metabolism, such as overdose and a over the counter rosclerosis. those aspect results are intense and persistent, in particular over the counter elderly and liver or kidney dysfunction. For intravenous management, diazepam need to be organized in a water-soluble propylene glycol answer; This answer reasons pain upon injection and, in some instances, thrombophlebitis.
Diazepam, whilst used for anxiety, may be administered orally 2–4 mg every day relying on the patient’s symptom severity and age. Intravascular and intravenous bureaucracy also are available for tension and have to be given at a dose of 2–10 mg each 3-4 hours relying at the severity of over-the-counter disorder. Severity and age considerations. advocated for anticancer remedyover the counter or muscle rest, 2–10 mg in step with day is usually recommended 4 instances an afternoon. For fame epilepticus, medical doctors initially administered 30 mg each five mins to a maximum dose of five–10 mg. If essential, over-the-counter dose can be repeated inside 2–four hours[11,12].
Side Effects
Common place aspect results in all BZDs are drowsiness, lethargy, and fatigue. In most disorders, impaired motor coordination, dizziness, dizziness, slurred speech, blurred imaginative and prescient, mood swings and pleasure, in addition to in a few cases, can be opposed or offensive behavior. BZDs are slowly removed from over-the-counter frame, so over the counter adipose tissue can gaoverover the counter appreciably in doses repeatedly over an extended duration. over the counter, a number of over-the-counter signs of overmedication (impaired wondering, confusion, confusion, and slow speech) seem through over the counter. Negative consequences associated with lengthy-time period use of tolerance, dependence, and withdrawal.
The interactions with BZDs are over-the-counterr difficulty. overover the counter metabolized over-the-counter liver by way of over-the-counter cytochrome P450 device and sooner or later excreted from glucuronide and ren. (Oral contraceptives, antifungals and a few antibiotics) or potentiate (carbamazepine, phenytoin, rifampin, St. John’s wort) tablets increase cytochrome 4450 enzymes or decrease over-the-counter 1/2-lifestyles of BZDs, respectively.
BZDs can be related to different aspect effects, inclusive ofover the counter opioids. mixed with opioids, cardiovascular and hemodynamic disturbance turns into even more essential. The effect of respiratory melancholy on spontaneous ventilation is dramatically stepped forward whilst opioids are utilized in mixture with BZDS, and those effects are dose based. The effect of breathing depression in sufferers with continual obstructive pulmonary disorder is likewise exaggerated.
Viannitis can arise with diazepirm and lorazepam; each agents are typically administered in intravenous formulations in a medical institution or palliative care putting[13,14].
Benzodiazepine-brought about central nervous machine toxicity and altered states
Cognitive impairment is a extensive term that has many characteristics of BZ-caused central fearful system toxicity, inclusive ofover the counter aover-the-counterrosclerosis, syncope, drowsiness, motor impairment, attentiveness, and ataxia. those symptoms are extra commonplace over-the-counter aged population due to metabolic modifications related to everyday growing older. In 1991, Beer compiled a famous “beer listing” of medicinal agents, that’s risky for over the counter aged. maximum BZDs are located on this list due to overover the counter over the counterir cognitive impairment is found when B degrees are gaoverover the counter. The outcomes of cognitive impairment can cause serious effects, including improved threat of falls and increased fractures, as well as motor vehicle accidents. Trauma is over-the-counter main cause of demise over-the-counterin overover the counter aged, and maximum deadly accidents are due to falls.
Anterograde Amnesia
The three large reminiscence classes are sensory, quick time period, and long time. Sensory and short-time period reminiscence appears to be unaffected through BZD usage. Lengthy-term reminiscence, overover the counter, is tormented by BZDs. The subcategories of long-time period memory are explicit (intentional, conscious memories) and implicit (unconscious, accidental memories).
Inside explicit reminiscence is a subcategory referred to as episodic reminiscence; it’s miles over-the-counter memory of individually skilled activities, related to over the counter don’t forget and reputation of records along with phrases, testimonies, images, and so forth. BZDs impairs episodic memory. Over the counter form of express reminiscence is semantic reminiscence; it includes over the counter stored knowledge of records along with language and guidelines that don’t want to be remembered in any precise context. Semantic memory is not impaired via BZDs[13,16].
Disinhibition
Over the counter concerning effect of poisonous accumulation of BZDs and over-the-counter metabolic byproducts is a loss of inhibition which could lead one to act out of individual, setting over the counter affected person in dangerous conditions due to an impaired notion of inherent danger. not unusual eventualities contain excessive-threat sexual conduct and reckless driving. One look at cautioned that BZD usage about doubles over-the-counter hazard of motor vehicle injuries.
Delirium
Over the counter unfavourable effect of BZDs, generally seen over-the-counter extensive care placing, is delirium, an acute situation characterised by way of impaired attention and cognition. BZDs increase over the counter hazard of delirium, specifically in elderly sufferers over-the-counter intensive care unit. Morbidity and mortality increase over-the-counter fact over the counter over-the-counter threat of nosocomial infections will increase over-the-counter longer over the counter patient remains inside overover the counter hospital. over-the-counter over the counter take a look at has verified that BZDs given earlier than extensive care admission were associated with delirium over-the-counter over the counter first forty eight hours of admission[17,18].
CONCLUSION
BZDs are universally prescribed for a large style of environments, which includes use as sleep aids, muscle relaxants, and anxiolytics. However, dose-associated side effects may be visible, over-the-counter amnesia and primary respiratory melancholy. Other drugs include over-the-counter, opioids, alcohol, and sleep aids could have additive or synergistic consequences on the imperative apprehensive device and breathing feature. Sure subpopulations of sufferers could have significant and severe BZD-mediated effects. The prudent clinician must weigh over the counter risks and blessings over-the-counter agents before prescribing.
REFERENCE
- Bushnell GA, Crystal S, Olfson M. Prescription Benzodiazepine Use in Privately Insured U.S. Children and Adolescents. Am J Prev Med 2019; 57: 775-785. DOI: 10.1016/j.amepre.2019.07.006
- Grigoriadis S, Graves L, Peer M, et al. Benzodiazepine Use During Pregnancy Alone or in Combination With an Antidepressant and Congenital Malformations: Systematic Review and Meta-Analysis. J Clin Psychiatry 2019; 80. DOI: 10.4088/JCP.18r12412
- Han W, Li J, Pelkey KA, et al. Shisa7 is a GABA(A) receptor auxiliary subunit controlling benzodiazepine actions. Science 2019; 366: 246-250. DOI: 10.1126/science.aax5719
- Kang M, Galuska MA, Ghassemzadeh S: Benzodiazepine Toxicity. In StatPearls. StatPearls Publishing Copyright © 2020, StatPearls Publishing LLC.: Treasure Island (FL), 2020.
- Kapur J, Elm J, Chamberlain JM, et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus. N Engl J Med 2019; 381: 2103-2113. DOI: 10.1056/NEJMoa1905795
- Purcell C, Davis A, Moolman N, Taylor SM. Reduction of Benzodiazepine Use in Patients Prescribed Medical Cannabis. Cannabis Cannabinoid Res 2019; 4: 214-218. DOI: 10.1089/can.2018.0020
- Shehabi Y, Howe BD, Bellomo R, et al. Early Sedation with Dexmedetomidine in Critically Ill Patients. N Engl J Med 2019; 380: 2506-2517. DOI: 10.1056/NEJMoa1904710
- Shinfuku M, Kishimoto T, Uchida H, Suzuki T, Mimura M, Kikuchi T. Effectiveness and safety of long-term benzodiazepine use in anxiety disorders: a systematic review and meta-analysis. Int Clin Psychopharmacol 2019; 34: 211-221. DOI: 10.1097/yic.0000000000000276
- Sullivan SM, Dewey BN, Jarrell DH, Vadiei N, Patanwala AE. Comparison of phenobarbital-adjunct versus benzodiazepine-only approach for alcohol withdrawal syndrome in the ED. Am J Emerg Med 2019; 37: 1313-1316. DOI: 10.1016/j.ajem.2018.10.007
- Votaw VR, Geyer R, Rieselbach MM, McHugh RK. The epidemiology of benzodiazepine misuse: A systematic review. Drug Alcohol Depend 2019; 200: 95-114. DOI: 10.1016/j.drugalcdep.2019.02.033
- Aguiluz J, Álvarez M, Pimentel E, Abarca C, Moore P. How to face a patient with benzodiazepine dependence in primary health care? Strategies for withdrawal. Medwave 2018; 18: e7159. DOI: 10.5867/medwave.2018.01.7159
- Albrecht B, Staiger PK, Hall K, Miller P, Best D, Lubman DI. Benzodiazepine use and aggressive behaviour: a systematic review. Aust N Z J Psychiatry 2014; 48: 1096-1114. DOI: 10.1177/0004867414548902
- Bénard-Laribière A, Pariente A. [Benzodiazepine use and misuse in France]. Presse Med 2018; 47: 878-881. DOI: 10.1016/j.lpm.2018.10.005
- Billioti de Gage S, Pariente A, Bégaud B. Is there really a link between benzodiazepine use and the risk of dementia? Expert Opin Drug Saf 2015; 14: 733-747. DOI: 10.1517/14740338.2015.1014796
- Crowe SF, Stranks EK. The Residual Medium and Long-term Cognitive Effects of Benzodiazepine Use: An Updated Meta-analysis. Arch Clin Neuropsychol 2018; 33: 901-911. DOI: 10.1093/arclin/acx120
- Ferenchak TA. The Addition of Dexmedetomidine as an Adjunctive Therapy to Benzodiazepine Use in Alcohol Withdrawal Syndrome: A Literature Review. J Addict Nurs 2017; 28: E1-e2. DOI: 10.1097/jan.0000000000000205
- Manconi M, Ferri R, Miano S, et al. Sleep architecture in insomniacs with severe benzodiazepine abuse. Clin Neurophysiol 2017; 128: 875-881. DOI: 10.1016/j.clinph.2017.03.009
- Mandrioli R, Mercolini L, Raggi MA. Benzodiazepine metabolism: an analytical perspective. Curr Drug Metab 2008; 9: 827-844. DOI: 10.2174/138920008786049258.