Ghugarkar Prasad Gorakshanath* & Preeti Khulbe
Gyan Vihar School of Pharmacy, Suresh Gyan Vihar University, Jaipur, India
ABSTRACT
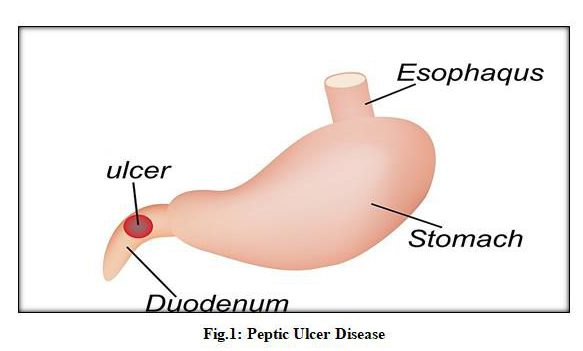
Peptic ulcer is a ulcer in the part of the side of GI Tracts in stomach or duodenum. Roughly 66% of patients found to have peptic ulcer illness are asymptomatic. Peptic ulcers are discovered to be because mainly of excessive amount of gastric acid, hydrochloric acid (HCL) and also because of pepsin and refluxed bile. In this article it is principally centered around Historical Background, Symptoms, Causes and Treatment of Gastrointestinal Ulcer. The purpose behind treating ulcers is to bring down the measure of gastric ulcer disease that your stomach makes, to kill the erosion that is made and to ensure the harmed territory so it can have the opportunity to mend. The fundamental point of this review article needs to sum up the ulcerogenic systems of different people associated with Peptic ulcer sickness.
Key-words: Duodenal Ulcer, Proton Pump Inhibitor, Gastric Acid, Stomach.
INTRODUCTION
Peptic ulcer infection gives gastrointestinal side effects like dyspepsia and can be hard to recognize clinically. It can have conceivably genuine complexities, for example, draining or hole, with a high danger of mortality [1]. It follows gastric mucosal wounds because of irregularity between the protective and the forceful components influencing the mucous [2]. The advancement of information with respect to etiopathogenesis of Gastrointestinal Ulcer illness from ulcerative driven sickness to an irresistible infection has opened up this subject for different examinations to locate the most ideal alternatives for the executives of this illness. The revelation of Helicobacter pylori has revealed incredible interest in the pretended by this organism. The annihilation of this living being has been discovered to be of vital significance to limit the inconveniences of peptic ulcers. The rate of peptic ulcer sickness has diminished as of late. This can mostly be clarified by the utilization of proton pump inhibitors (PPIs) and destruction treatment for Helicobacter pylori. But, peptic ulcer difficulty, including hole, a significant medical services issue. This might be identified with expanded utilization of non-steroidal anti-inflammatory drugs (NSAIDs) and to the increasing populace [3,4]. Pervasiveness of peptic ulcer has diminished from recent years essentially because of a powerful treatment of H. pylori disease destruction, anyway broad utilization of NSAIDs and acetylsalicylic acid causes certain gastrointestinal complexities. NSAIDs and ibuprofen may lead towards gastrointestinal mucosal injury, and consequently the inconveniences. Different medication regimens accessible incorporate proton pump inhibitors (PPIs) fundamentally utilized. [5,6]
History of GI Ulcer
Peptic ulcer infection is not a new it was notable in ancient times also. It is not clear that when first clinical history was reported and diagnosed [7]. It may be viewed as the primary medical procedure for a gastric or peptic ulcer was draft by Goldstein. Along with, he fled, yet they got and attached him to the doorknocker. At that point Asklepios opened his stomach, removed the ulcer, closed him up once more, and loosed his bonds. The post-mortem examination indicated a plainly noticeable punctured prepyloric ulcer bringing about intense diffuse peritonitis muddled by scattered coagulopathy [8]. So much for peptic ulcer as an advanced sickness.
Duodenal Ulcer
It is in the territory of duodenal ulcer illness that the conventional acid peptic hypothesis holds the entirety of its legitimacy. There are numerous solid contentions supporting the significant part of hydrochloric acid in the causation of duodenal ulcer. It is notable that duodenal ulcers basically never happen except if the gastric mucosa can discharge at rent significant measures of HCI. Ulcers in the duodenum or in the gastric source zone are promptly actuated in test creatures by measure intended to enlarge apparently the gastric yield of HCI [9].
Gastric Ulcer
This piece of tile conversation will manage the substance off ongoing gastric ulceration. It should be called attention to at the beginning that the term gastric ulcer is marginally deceptive. Late examinations have uncovered that constant gastric ulcers consistently create in the antral mucosa and just hardly the parietal organ zone. It must, obviously, be understood, that there is certifiably not a fixed connection between the antrum and the fundus of the stomach. With age and intestinalization of the gastric mucosa, the outside of the parietal organ region progressively diminishes [10].
Symptoms
Most of the patients does not show or don’t have side effects. Indications of gastric ulcers are Burning stomach torment, sensation of completion, swelling or burping, Intolerance to greasy nourishments, acidity or hyperacidity and vomiting, in some patients loss of weight also seen.[11,12]
Causes
Having these microscopic organisms filling in your stomach can harm the bodily fluid covering that secures the tissues coating the stomach and duodenum. This permits stomach corrosive to come into contact with the layering, causing irritation and ulcers. The microscopic organisms additionally animate gastric cells to fill in the coating of the duodenum, discharging corrosive and pepsin. In the U.S., 30% to 40% of the populace is tainted with H. pylori, yet most never build up a ulcer. The microscopic organisms can be spread by means of salivation, food, water, and eating utensils. It is frequently procured in youth with no indications. [13]
Long haul utilization of non-steroidal mitigating drugs (NSAIDs) is another basic reason for peptic ulcers, raising your danger multiple times that of non-clients. These incorporate over-the-counter items containing anti-inflammatory medicine, ibuprofen, and naproxen sodium. Remedy NSAIDs are likewise used to treat a few joint conditions. NSAIDs can cause the stomach’s guard instruments to come up short in two or three distinct manners. They can make the stomach powerless against the destructive impacts of sour and pepsin by meddling with the stomach’s capacity to deliver bodily fluid and bicarbonate. This characteristic bicarbonate typically kills stomach related liquids and separates them into less unsafe substances. They can likewise influence cell fix (by restraining the COX-1 receptors) and blood stream to the stomach, which regularly help secure it. [14]
Diagnosis
It is mainly diagnosed by Endoscopic Inspection of Upper Gastrointestinal Tract. The specialist will cautiously take care of the inspection of patients throat part and into stomach and GI Part of duodenum. A small camera which is attached in lower section of Endoscope will send the picture and details of GI region. It also uses air so as to visualise it easily. The endoscope siphons air into your stomach and duodenum, making them simpler to see. [15]
Treatment of GI Ulcer
Since their presentation into clinical practice in the last part of the 1980s, proton pump inhibitors (PPIs) have significantly changed the way to deal with peptic ulcer infection the board. PPIs remain the backbone of clinical treatment for peptic ulcer-related gastrointestinal dying. Very much performed efficient surveys uphold the inception of PPIs before endoscopic assessment for intense upper gastrointestinal dying, albeit an unmistakable mortality advantage has not been illustrated. The length of PPI organization following the conclusion of a peptic ulcer relies upon the basic ulcer etiology, area, and related difficulties. A definitive objective of PPI treatment is to advance ulcer mending through sour concealment, while the basic etiology of the ulcer(s) is tended to. Proton-siphon inhibitors (PPIs) are individuals from a class of drugs whose principal activity is a significant and drawn out decrease of stomach acid creation. Inside the class of drugs, PPI ties covalently to the gastric H+, K+-ATPase by means of disulfide bond. Cys813 is the essential site liable for the restraint of acid pump protein, where PPIs bounds. [16,17]
REFERENCE
- Sung JJ, Kuipers EJ, El-Serag HB. Systematic review: the global incidence and prevalence of peptic ulcer disease. Aliment Pharmocol Ther 2009; 29:938-46. 10.1111/j.1365-2036.2009. 03960.x 19220208.
- Ramakrishnan K, Salinas RC. Peptic ulcer disease. Am Fam Physician. 2007;76(7):1005-12.
- Sung JJ, Kuipers EJ, El-Serag HB. Systematic review: the global incidence and prevalence of peptic ulcer disease. Aliment PharmacolTher. 2009; 29:938–946.
- Soreide K, Thorsen K, Soreide JA. Strategies to improve the outcome of emergency surgery for perforated peptic ulcer. Br J Surg. 2014;101: e51–e64.
- Lau JY, Sung J, Hill C, et al. Systematic Review of Epidemiology of Complicated Peptic Ulcer Disease: Incidence, Recurrence, Risk factors and Mortality. Digestion. 2011; 84:102‒113.
- Drini M. Peptic ulcer disease and non‒steroidal anti‒inflammatory drugs. Australian prescriber. 2017;40(3):91‒93.
- Goldstein HI. The use of magnesium trisilicate colloidal kaolin and aluminium hydroxide in acid gastric therapy: Historical notes on ulcer of the stomach and duodenum. J Internal Coll Surgeons 1939; 2: 379-408.
- Brinton W. On the pathology, symptoms and treatment of ulcer of the stomach. London: John Churchill, 1857.
- Morrissey JF, Tanaka Y, Thorsen WB. Gastroscopy, A review of the English and Japanese literature. Gastroenterology 53: 456, 1967.
- Eaton SB, Fleischli DJ, Pollard JJ, Nebesar RA, Potsaid MS: Comparison of current radiologic approaches to the diagnosis of pancreatic disease, New Eng. J Med 279: 389, 1968.
- Leslie W. Peptic Ulcer: Reappraisal of peptic aetiology, Ann Roy Coll Surge Engl 1972;50:146-163.
- Crispian S. Rosemary S. Review on Ulcer Br Med J 2000;321 : 162-165.
- Testerman TL, Morris J. Beyond the stomach: an updated view of Helicobacter pylori pathogenesis, diagnosis, and treatment. World J Gastroenterol. 2014;20(36):12781-808. doi:10.3748/wjg. v20.i36.12781
- Ramakrishnan K, Salinas RC. Peptic ulcer disease. Am Fam Physician. 2007;76(7):1005-12.
- Steingoetter A, Fox M, Treier R, Weishaupt D, Marincek B, Boesiger P, Fried M, Schwizer W. 2006. Effects of posture on the physiology of gastric emptying: A magnetic resonance imaging study. Scand J Gastroenterol 41:1155–1164.
- Ramakrishnan K; Salinas RC. (2007). Peptic ulcer disease. Am Fam Physician. 76(7): 1005-1012.
- Pilbrant A. And Cederberg C. – Development of an oral formulation of omeprazole. – Scand. J. Gastroenterol., 20,113- 120, 1985.